Sparky
Well-Known Member
Radiology Report
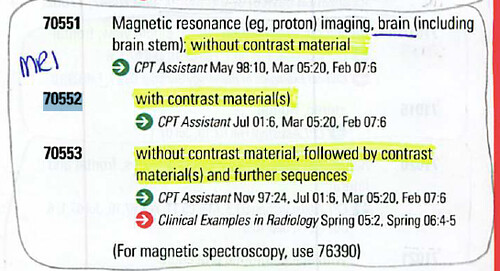
EXAMINATION: MRI of brain with contrast
CLINICAL SYMPTOMS: Slurred speech, right arm weakness
MAGNETIC RESONANCE EXAMINATION OF THE BRAIN was performed prior to contrast
utilizing T1-weighted sagittal views as well as spin density and T2-weighted sequences in the axial plane. These were supplemented with axial T1-weighted sequence following intravenous infusion of paramagnetic contrast material. Diffusion sequence was also performed.
In the spin density and T2-weighted sequences (images 17 and 18 of series 3), there is a small localized area of occipital cortex that shows increased intensity. This is also bright in the diffusion sequence. This area is not hyperintense in the ADC map.
I do not appreciate significant abnormal increased or decreased intensity within
brain parenchyma of the remainder of the supratentorial brain. However, there is
bilateral irregularly shaped increased intensity within the pontine tegmentum. This
is not hyperintense in the diffusion sequence. Ventricles are of normal size. Normal gray-white matter delineation. No abnormal contrast enhancement of brain parenchyma.
IMPRESSION: Small hyperintense area of the cortex of the right occipital lobe, as
described above. This is also hyperintense in the diffusion sequence but not in the
ADC map. This would indicate that this represents limited subacute infarction. I do
not appreciate other areas of subacute infarction. Remainder of supratentorial portion
of the brain is unremarkable. Hazy increased intensity within the pontine tegmentum. This is not unusual in the older age group (8th and 9th decades) and is sometimes thought to represent evidence of microvascular ischemic change. However, it is rarely indeterminate. In this
case, I do not appreciate evidence of enlargement of the brainstem, nor is there
abnormal enhancement to suggest neoplasm. I cannot elucidate further.
Answer: CPT Code: 70552 (Comments: Incorrect code)
EXAMINATION: MRI of brain with contrast
CLINICAL SYMPTOMS: Slurred speech, right arm weakness
MAGNETIC RESONANCE EXAMINATION OF THE BRAIN was performed prior to contrast
utilizing T1-weighted sagittal views as well as spin density and T2-weighted sequences in the axial plane. These were supplemented with axial T1-weighted sequence following intravenous infusion of paramagnetic contrast material. Diffusion sequence was also performed.
In the spin density and T2-weighted sequences (images 17 and 18 of series 3), there is a small localized area of occipital cortex that shows increased intensity. This is also bright in the diffusion sequence. This area is not hyperintense in the ADC map.
I do not appreciate significant abnormal increased or decreased intensity within
brain parenchyma of the remainder of the supratentorial brain. However, there is
bilateral irregularly shaped increased intensity within the pontine tegmentum. This
is not hyperintense in the diffusion sequence. Ventricles are of normal size. Normal gray-white matter delineation. No abnormal contrast enhancement of brain parenchyma.
IMPRESSION: Small hyperintense area of the cortex of the right occipital lobe, as
described above. This is also hyperintense in the diffusion sequence but not in the
ADC map. This would indicate that this represents limited subacute infarction. I do
not appreciate other areas of subacute infarction. Remainder of supratentorial portion
of the brain is unremarkable. Hazy increased intensity within the pontine tegmentum. This is not unusual in the older age group (8th and 9th decades) and is sometimes thought to represent evidence of microvascular ischemic change. However, it is rarely indeterminate. In this
case, I do not appreciate evidence of enlargement of the brainstem, nor is there
abnormal enhancement to suggest neoplasm. I cannot elucidate further.
Answer: CPT Code: 70552 (Comments: Incorrect code)