- Introduction
- ICD-10 2023 April Update
- New Codes
- S00-T88
- V00-Y99
- Z00-Z99 Health Literacy
- ICD-10-PCS Med/Surg
- ICD-10-PCS Administration
- ICD-10-PCS New Tech
- Submit Your Topic Requests
Introduction
Hello everyone. We’re ready for another Live with CCO. And of course with our Live with CCO’s, it’s a little more casual. Feel free to ask questions. I’ll keep an eye on both of the monitors as we move forward with our topic.
ICD-10 2023 April Update
Great topic. The ICD updates for 2023. Now, we’ve already done the regular updates that we get at the end of every year, but now they have started something new. So for the 2023 April updates, we have ICD-10 and in CM and PCS, the new code.
New Codes
Remember, again back. Now you can start saying, back in the olden days we got an update every year and that was for all of the code sets and you knew when the updates were gonna be launched and everybody started pushing to get educated on the new codes and it was honestly, it’s a great marketing tool to get people interested in what services that you can offer, but now we get an update on codes twice a year, April 1st, 2023.
The new codes went into effect for an additional update. This started when they did something dramatic in the middle of the year. They created a code for COVID-19 and they launched a new code to track that and then when they did that they just hacked in another code for vaping, and because I guess they had that one ready to go, ready to launch. Well, it worked so well that they did it again and then they did it again. So now, we probably are going to have that happen in the future. You know, they start something like that new then it’s kind of hard for them to take it away from you.
There is some interesting updates. But for the most part, I think what you’re going to see in these what I’m going to start calling mid year updates or April updates is clarification, expansions and you’ll notice that as we go through what’s being updated that went into effect in April that they expanded existing codes. Honestly, they didn’t come out with new wild crazy codes. What they did was they decided to expand and give kind of a higher definition to some existing codes.
Hi guys. I see people doing shoutouts and lookie there, Joanne’s here. Joanna’s a former CCO instructor. Good to see you. Hello, everybody. So let’s talk about what is available in these updates. And as we talk about those, it’s really pertinent to consider why? Why did they do these codes? In the you know in the first place, why do we have these codes? They don’t create codes unless they’re needed, and you hear me say this over and over again. It’s kind of a mantra. We code for statistical purposes. It happens to be a convenient way to get paid knowing that. It’s the statistics. It’s all about what we’re trying to track. When you see a completely new code being developed and introduced that isn’t like anything that you’ve seen before, a new diagnosis, et cetera, then that tells you there is absolutely a need for tracking that diagnosis at the same time as CPT.
Now we’re going to be doing ICD 10, both CM and PCs tonight to talk about the updates that were introduced for April 1st, 2023. You guys know I’m a huge fan of diagnosis codes. ICD-10-CM is my favorite code set. Number two favorite, of course, is ICD 10 PCS. My hope is that PCS is going to replace CPT. It’s a much better code set and it doesn’t have a monopoly on it being owned by the AMA. Again, I’ve said that several times, so just mark my words, let’s see how long it takes to take over. I predict within the next five years, maybe less. I CD-10-,CM how many new codes do they have? They have 42 new codes that we’re going to look at. And with PCs, we have 34 codes now. I am not going to pull out every single code and let you see them. You can look those up. You’ve probably already been looking at them.
What I’m gonna talk about is the descriptions for the codes, so that’ll help us understand it a little more. We’re not going to spend a lot of time again just talking about and reciting kind of droning out what the codes are.
S00-T88
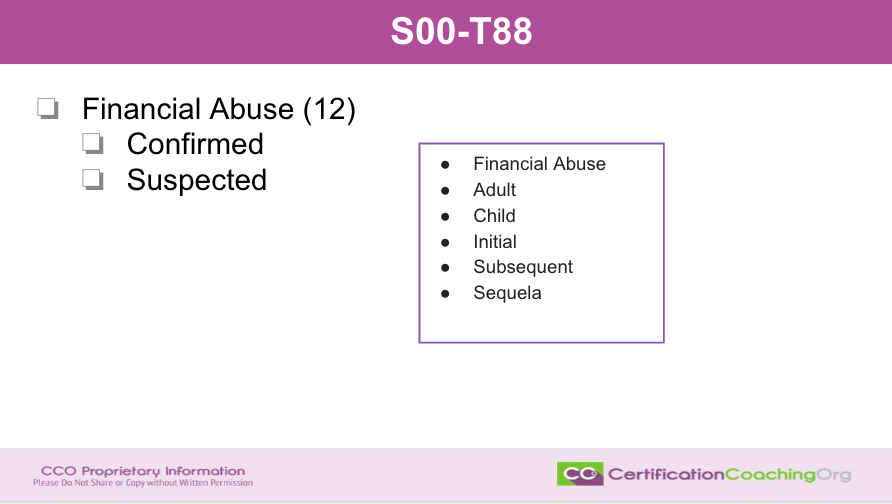
The first area that we’re going to look at is ICD-10-CM. The code range is S00 through T88 and these are codes for financial abuse. They have already been developed. You’ll probably see some of these maybe already have used some of these codes. But, they’ve expanded them. There’s 12 codes. The reason you’re going to see 12 codes for financial abuse is they have for confirmed and suspected and then who is the financial abuse? Who is causing the financial abuse, not who’s it happening to, because that’s defined as the patient. But what’s the source of the financial abuse and it’s divided up into adult, child and then initial, subsequent and sequela or late effect. It will not take long to get 12 codes out of financial abuse. Relatively new that we would be tracking that and isn’t that odd because is financial abuse a diagnosis, right? So, I thought that one out of all of the other ones that we’re going to be talking about. Was a little skeptical.
However, I can tell to you that we have a son that’s disabled and he just turned 18. And so, one of the things that you do when you have a disabled child is that you can choose to get guardianship over them. And because they’re an adult, doesn’t matter what their mental capacity is, they are by law, an adult. And so, when we went to the lawyer and they talked about it, one of the things that is problematic and the reason you go to the court and have to petition for guardianship is the financial abuse that happens because if a person is on disability, they get income and that income can be abused. In other words, the lawyer said, you know, they could put you in a basement and just cash your checks. You know, someone could do that.
So ,it’s overseen by the court, and if you have guardianship over someone, you have to show where that money is coming in and where it’s going and so on and so on. Maybe it has to do with that I wasn’t sure, but it seemed a little odd for it to be a diagnosis code, financial abuse. However, abuse is abuse, right? That is a diagnosis, and it could also contribute to other diagnoses, right, depression and so on, and so forth. And I’m sure you can think of other things that if you, you know, contemplate it a little bit, how that would kind of spark other types of scenarios that a patient might be suffering. So, keep in mind financial abuse, we’re able to track that. It’s confirmed or suspected and then child or adult, and then is an initial subsequent or sequela. There’s 12 codes ultimately.
V00-Y99
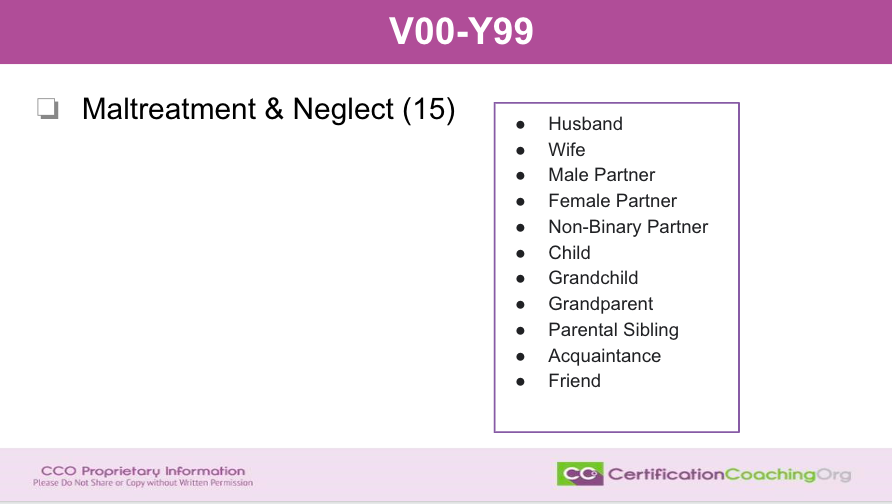
Now, these codes were a little more familiar with V00 through V or Y99. They have 15 new codes for maltreatment and neglect. Now, when I say they have new codes, there were existing codes already for maltreatment and neglect. They have expanded those and so when you look at them, you may think, oh, wait a minute. I thought we already had this code well. That’s not what we’re talking about. They will, when they create a new code or break up a code to define it and split it, they will delete the original code and expand the characters. So, this code is deleted because you got a new code with this code with additional characters.
So, let’s talk about maltreatment and neglect and there’s 15 codes. So, the way that’s divided up is is the uh, maltreatment or neglect by the husband, the wife then they have a male or female partner. Again, husband or wife would be like. So, you would have a document stating that you know you have legally married. Then you have male partner, female partner, non binary partner was added, child and child, grandparent. We have parental sibling acquaintance and friend. This is interesting because we don’t always think about all of the categories that could be considered maltreatment or neglect. Maltreatment is very broad. A very, very broad term and they expanded a little bit more with the definitions of these codes and again 15 codes that we’re looking at.
Z00-Z99 Health Literacy
I really personally appreciated this new code that’s come out for health literacy. Again, because if I have a child that doesn’t have the capability of reading then he would be health illiterate and the definition of this onen ew code that’s in the code range Z00 through Z99 is that the patient cannot find, understand or use information and services to make health related decisions. And of course, he would not be able to do that because he can’t read and he doesn’t have the ability to write. So, this makes perfect sense. We would want to be able to track that in our patients and as we’re tracking, we also have to think about the medical decision making that goes along with this. All of our diagnosis, all the diagnosis that a patient has we, you know, it doesn’t necessarily mean that a person is sick, right, or even if they have chronic conditions, acute conditions. But the medical decision making is going to go up for a patient that is health, has health literacy problems. They’re not going to be a good historian. There is going to be medical decision making that’s going to be needed from the provider as well as probably a team working with that patient. So again, I really thought this was brilliant, that they have gotten this new code.
Physical Environment
The next code is going to be physical environments where patients, there’s two new codes and the patient services are unavailable in the patient’s physical environment and other issues with the environment. This could include the example that was given as lack of sanitation in the patients home. I always think of those shows “Hoarder”, you know. Remember when I don’t know maybe that’s still out. But if you have a lack of sanitation in a home, then again that physical environment is affected. If you have a diabetic patient that is not maybe geriatric diabetic patient that also has osteoporosis and then we think about, you know, stubbing their toe. You know, if you’re a normal, healthy patient with no other, you know mid-age, that’s not a big deal, but if you’re a diabetic patient that can be problematic. And so, having lack of sanitation in the home, again, this is just one example. They do expand it a little bit more with some other definitions of financial hardship. So, physical environment, 2 new codes that have been implemented for April.
Inadequate Housing
The next one is that these codes already existed, but they expanded them into inadequate housing. Now included in that for inadequate housing is temperature in the home. So, I know that when we lived in Texas that at one point we lived in a more western part of Texas and it was hot. Very, very hot and therefore it, you know, could be a problem for people that didn’t have air conditioning and central air. When you have temperatures that stay for days over 100 degrees, 100 to 103 degrees then it if you’re in a home, especially if it has poor air circulation and you’re gonna be hard pressed to find a home in Texas at West TX that doesn’t have good ventilation, but because it just probably wouldn’t be built without that. In the event though that, you know, a fan may not be adequate, you’re going to need a temperature control.
And on the other side of that, the cold temperature. When we lived in Rochester, MN for a year, we were told that that was one of the mildest winters they’d ever had, which was really good because they make you go out and play when it’s 20, you know if it’s colder than 20 below then you don’t have to go outside and play in there for recess. But again, they’re used to cold weather up there. If you don’t have proper heating or for some reason say you’re not able to pay the gas to heat their home because of the expense of the gas that we all know that’s gone up then again, the temperature in the home could be affected. Inadequate housing will cause health issues.
Utilities in the home. If you don’t have adequate utilities and unspecified inadequate housing. Remember, and other inadequate housing. What do we define that as? Unspecified means either we don’t know for nor right the provider doesn’t know for sure or when we look at the other codes, more testing needs to be done or OK, we’re aware that the providers are aware that there’s inadequate housing. We don’t know all of the details, but they are aware of it. And then others are defined as they’ve identified the inadequate housing although it doesn’t fall, there’s not a code for the specificity that’s being given. And so in the documentation, we would want to see what the inadequate housing was represented by and then you would use the code for others. Again, 4 new codes for inadequate housing and some of those have been deleted because they expanded the definitions for those. Oh, sorry, I’m starting to flip the wrong slide.
Patient Non-Compliance
Next, we have patient non-compliance. Now, we have had patient non-compliance codes for a while. This would include medication and renal dialysis. However, what they did was they expanded it. Are they non compliant because of financial hardship or is there other reasons other than financial hardship? Again, if we use a code for other, we need to have in the documentation what the other is defined as. We can’t just say other. They’re going to audit that and they need a description of what the other is. And then as more as time goes on, we may see more defined patient, non-compliant terms. I really appreciate these codes being expanded and. Added again, some of them feel a little confusing, but when you are noodle on it a little bit, you think, oh yeah, ok. I see why this would affect medical decision making for our providers.
How are they going to work around the hardship of a patient that needs renal dialysis that can’t get to the clinics For dialysis because they don’t have a. They don’t have the money to get an Uber, and they don’t have a support system as far as the friends and family that has the ability to get them there. This would be a patient not being compliant, not by choice, but because of a financial hardship. So, I think that is, oh, and medical reasons such as Joanna says, depression, this would definitely lead into other codes. You can see how they piggyback on each other to tell the full story of the complexity of medical decision making that’s happening with these particular patients. And we don’t want to state that they are non-compliant when there is a reason for their non-compliance. Because, I know that when I see that in the documentation or I see that code, you automatically have assumptions that they’re just not taking their medication or they’re diabetic and they’re not controlling their diet or you know. No, it may be something else. And now we’re able to define it and get resources if we track it, then we’ll be able to get resources.
ICD-10-PCS Med/Surg
Heart and Great Vessel
Let’s move into the codes for ICD-10-PCS. Brilliant code set, of course. Medina says for those of us who are testing in June, well, we need to purchase new 2023 manuals due to these updates? No, you will not. The good news. Excellent question. Thank you for asking that. You can print the changes and you’re allowed to bring those in when you test. They will not be in the new manual in the 2023 manuals. They will be in the 24 manuals, but you’re able to make either notes in your manuals regarding the additions, the expansions. Most likely though, because the tests are already written, so these codes are not going to most likely be involved in testing scenarios. However, they could. They could be. But if you are ever concerned, you can always reach out to the proctor that is going to be doing your testing and they’ll be able to give you details or let them know. You know. I’m aware of the new codes. What should I do? Am I going to be writing these in my manual or can I bring this piece of paper that states the new update codes and they’ll be able to tell you what their policies are.
Again, it depends who you’re testing with. AHIMA versus AAPC or for other credentialing organizations, they may all have different rules. AHIMA doesn’t let you write in your manuals. So again, check with who the Proctor is going to be beforehand, just to be sure, and usually proctors will send you out an e-mail ahead of time to make sure you have all the details about where you’re going, what time to be there and what to expect, and stuff the local chapters are pretty good. Both AHIMA works with the people that are getting ready to test. They have chapters as well. Very good, excellent question. Thank you for saying that.
Moving on to our ICD-10-PCS. Again, PCS is set up a little differently and there was only one new code in the heart and great vessels vessel area and that code is going to cover the occlusion of a thoracic aorta using a temporary intraluminal device. Now, this is an open approach and the previous code, they only did percutaneous or percutaneous endoscopic. Now, they have the option for an open approach. Very good. Obviously they needed that to be expanded. This makes perfect sense to you if you deal with PCS codes. If you don’t, you’re probably looking at that and uh, I don’t get it. I am not explaining the code set or how the codes work. I just want to give you an update so that you can go out and look at these codes and do a little on your own, get to love those manuals some more.
In the Med/Surg also, for lower arteries we have a new code for again the occlusion of the abdominal aorta and that is the same thing they added the open approach to the procedure. They didn’t have that before. So, very good that they expanded those.
Upper Bones
Then we move on. 6 new codes were added for upper bones, the upper bones. I love the bones. 6 new codes that are destruction and I on the other slides I actually made that bold. What they were doing, so destruction on this one, I forgot to to highlight that for the root operation as well. I was trying to get out and it was slipping in my brain. This one is going to be 6 new codes for cervical and thoracic vertebra with laser interstitial thermal therapy or LITT and this is open approach, cutaneous or percutaneous endoscopic approach. What they did was CMS added the LITT to the upper bone destruction table, and then there’s a qualifier to capture the cases that specifically use the technology for the LITT. So, good to know that that’s been expanded.
Lower Bones
That one was new to me. I knew very little well about that, but if they do, the upper bones, that means they got to do the lower bones. So, the same thing was done. That was expanded for bone destruction in the bone destruction table.
ICD-10-PCS Administration
Moving on now to administration and within administration and the circulatory system, they have 14 new codes that were added to the transfusion and this is going to be the same verbiage they use every time, whole blood serum albumin, frozen or fresh plasma, frozen or fresh red blood cells and platelets, and they put that into the bone marrow. So CMS, what they did was they went ahead and added the region of bone marrow to the administration table. And, they gave an example of the intraosseous and I’m not sure if I said that right, but again, they’re putting it into the bone marrow administration of blood products. And it’s interesting that some of these codes are a little slow to update because they are doing some pretty amazing things with bone marrow right now and stem cells.
ICD-10-PCS New Tech
Then New Tech. New Tech is the last area that had additions for introduction. There’s one new code that is the introduction of reg-cov2 and it is an antibiotic. And what they did is they added this extension so that they’ll enable the efficient tracking of therapeutic use when treating COVID-19. There’s additional ones for this.
Again, they’re tracking COVID-19. Very, very detailed. They can track with CPT and they can track with PCS as well. So, there’s three new codes for the introduction of this other medication which I am not going to try to, I’m not even going to try to say what that is. S-A-B-I-Z-A-B-U-L-I-N. Good luck with that. I’m sure there is some kind of nifty little abbreviation, but it’s an antiviral, anti-inflammatory therapeutic. And so again, they’re tracking the administration or the giving of this medication with these PCS New Tech additions.
Then, I don’t know I think this may be the last one. 2 new codes. Again, introduction for another. They’re administering this. This has nothing to do with COVID, but it is another big giant word. Exagamglogene autotemcell. I’m sure that someone who deals with this is laughing right now. It actually is cells like stem cells, but they’re modified and they’re using those to treat sickle cell. Pretty fascinating. I mentioned before that they’re doing a lot of stuff with stem cells and treated cells reintroducing them into the body and being able to rejuvenate joints and other things and again, it’s it’s kind of fascinating. I mean, they’ve been doing this for a while, but I thought it was pretty fascinating and we’re gonna start seeing more and more of these CPT codes pop up HCPCS and things, too. So, this Exa-cell, isn’t that funny? It’s also known as CTX001. Yeah, and it’s like a stem cell transplant procedure. So, pretty cool.
Submit Your Topic Requests
That’s it, guys. Now, if you have a particular area that you’re dealing with, maybe at work or as a student and you’d like for us to do the research and kind of unpack it for you, feel free to send in a topic request. We listen to you. We want to give value to what we do and the best way to do that is to kind of get a feel for what the needs are because if you don’t give topic requests, we’ll always talk about ICD-10. Because that’s what I enjoy the most. So, you don’t want to have that happen to you, do you? Maybe you enjoy it, too. I don’t know. But if there’s an area that you want us to do a webinar on and give additional training on then you can submit that request very easily. Go to https://www.cco.us/topic-request and we’ll get right on it. We like to plan ahead and some of the things that we request we get take a little bit more time. I have to check in with my peers and get the details and figure out the best way to present it. So, that’s easy. It flows easily, right?
But if it has something to do with the disease process or ICD-10 or even PCS, then I can regurgitate knowledge all day long. Then it goes to other topics that may have to do a little or a risk adjustment, too. You know how much I love risk adjustment. So, we really appreciate you sending in topic requests. So, at this note again what the needs are. I do know for a fact that if you are also a club member, you always take priority. So, we go through all the requests from the club members first and then we branch out to other requests that come in. Just letting you know they get preferential treatment.
Let’s see, Debbie says. “Is there a list we can download for the new codes?” Yes, it’s on CMS.gov. and I also bookmarked it for you right there. Thanks, guys. Don’t forget you can comment and share this. OK. Bye guys.